Athor: Sarosh P. Batlivala, MD, MSCI, FPICS
Date: 31-Oct-2023
How I do it: Tips, Tricks, and Techniques
A PICS Society Education Series
How Do I Close Systemic-to-Pulmonary Artery
Collaterals using Microparticles?
Introduction:
Pediatric and congenital interventional cardiologists deal with many patients who have systemic-to-pulmonary artery collaterals (SPC). These SPCs are common in patients with single-ventricle physiology and chronic hypoxemia. Though the SPCs increase pulmonary blood flow, they are also volume loading because much of the flow is ineffective. Since these networks arise from normal arteries (e.g., internal mammary, intercostals, etc.), traditional treatment has involved coil occlusion of the feeding vessel. However, SPCs can redevelop from those vessels, distal to the coils, which makes ongoing treatment difficult if not impossible. Further, a general principle for optimal vessel closure is to occlude as distally as possible. Particle occlusion can therefore be a strong alternative since the feeding vessel remains patent and the particles occlude the distal SPC connection to the PAs (1).
Anticipated challenges of the procedure:
Given the flow-directed nature of particle delivery, the catheter must be securely positioned well into the feeding vessel. Back flow of particles into a major systemic or CNS-supplying artery can have devastating consequences. As above, common feeding arteries arise from:
- Subclavian system (common) = Internal mammary, Thyrocervical trunk, Lateral thoracic
- Coronary arteries
- Thoracic Aorta (common) = Intercostal, Bronchial
- Abdominal aorta = phrenic, celiac plexus branches
The artery of Adamkiewicz is particularly noteworthy. This vessel is the primary arterial supply for the thoracolumbar spinal cord so occlusion can lead to spinal cord ischemia and paraplegia. Moreover, this vessel can arise from any of the intercostal arteries so interventionalists need to obtain clear angiograms of intercostal arteries to ensure this artery is not arising from a vessel intended for particle occlusion.
Tip 1. Planning and Preparation
- Know your patient's anatomy (obviously!)
- Understand how to grade SPC flow:
- Pre-catheterization MRI can provide quantitative data
- Angiography (1):
- mild = only the segmental PA branches opacified
- moderate = proximal PA (i.e., RPA or LPA) opacified
- severe = contrast refluxes back into MPA or contralateral PA.
- Develop an algorithm/treatment protocol to establish thresholds
for SPC occlusion. Such an algorithm can take the following factors into
account
- Threshold % of aortic outflow (e.g., 30% or 40% SPC flow)
- Angiographic grade
- Systemic ventricular EDp
- Cardiac chamber dilation
- Planned operation(s) and timing
- Systemic saturation
- Hemoptysis (often an independent indication)
- Histopathologic data demonstrated SPC diameter (median) in Fontan patients ≈160 µm (1).
- Occlusion induces an inflammatory response, which triggers ongoing SPC development; SPC flow may return to baseline and even exceed it approximately 6-8 weeks after embolization. So if performing SPC occlusion as part of a pre-operative assessment and preparation (e.g., pre-Fontan), the surgery should ideally be scheduled within a month of the particle occlusion procedure (2).
Tip 2. Tools needed
- A separate cart for all the particle equipment is recommended. This will ensure that stray particles do not contaminate the primary procedural and supply tables, minimizing the risk of inadvertently injecting particles into the patient non-selectively.
- Catheters:
- "Guide" catheter – a standard 4Fr catheter, 0.038" lumen (e.g., Bentson/JB, JR, Glide, etc.). This catheter engages the feeding artery for angiography and is a guide for the microcatheter through which the particles are delivered. If this catheter is engaged deeply enough, particles can be delivered directly through this catheter as well.
- Microcatheter – Various options, need to ensure the lumen diameter is able to accept the specific microparticles (see particle manufacturer website, which often recommends appropriate microcatheters). We do not endorse a particular product, but the 2.8Fr Cantata (Cook®, Bloomington, IN USA) and Renegade Hi-Flo (Boston Scientific®, Marlborough, MA USA) microcatheters work well.
- Particles (two types)
- Polyvinyl alcohol = Irregular shape, grouped by sizes (produced by pulverizing PVA then passing through sifts of different sizes). Suggest minimum size of 500 µm (we use 500-710 µm). Sizes >1000 µm may be challenging to deliver given larger requisite microcatheter.
- Tris‑acryl gelatin = precisely engineered micro-spheres; care must be taken as agitation can disrupt/destroy the particles
- Other Equipment (Figure 1)
- Fresh surgical towels
- Hemostatic Y-adaptor (model of operator preference)
- Three-way stopcock (low or high pressure)
- Syringes: 10mL (suggest at least four - two for angiography and two as particle slurry "reservoirs"), two 1 or 3mL syringes for particle delivery
- Three bowls/sterile cups – one each for flush, contrast, and the particle slurry
- Flush and contrast (~50mL to start) specifically for the additional procedural table
Tip 3. How I do it
- Once baseline, non-selective angiography demonstrates a significant degree of SPCs, and the decision is made to occlude them after the diagnostic assessment, obtain all requisite equipment so that occlusion can be performed expediently.
- Set up the particle table. Obtain flush and contrast as above. Label two 10mL syringes for contrast injection, and two 10mL syringes to serve as particle reservoirs, and two 1- or 3mL syringes for particle delivery. Obtain a vial of particles. Empty the particles into a clean sterile cup and add 20mL of contrast and 2mL of flush. Stir the mixture and withdraw 5-10mL into a reservoir syringe. Hold the syringe steadily in a vertical position for at least 10 seconds and observe for particle aggregation. The goal is to achieve a suspension. If the particles begin to float, the injectate is too dense and if the particles sink then the injectate is not dense enough. In those cases, empty the contents back into the particle slurry cup and add 1-2mL of contrast (to make the injectate more dense if the particles were sinking) or 1-2mL of flush (to thin the injectate if the particles were floating). Repeat this process as many times as necessary until a suspension is achieved.
- Fill the reservoir syringe with the 8-9mL of particle slurry and attach to a 3-way stopcock (position per operator comfort). Attach an empty 1 or 3mL syringe to the other port.
- Obtain microcatheter and prepare for use.
- Selective angiography in the feeding vessel(s) should be performed first. This angiogram is typically performed with the guiding catheter (noted above). Save a select frame as a roadmap; this frame should demonstrate the origin of the feeding vessel from the major systemic artery (e.g., the internal mammary and subclavian artery junction) (Figure 2).
- If the guiding catheter is sufficiently deep in the vessel intended for occlusion, particles can be delivered directly through the 4Fr catheter into the main feeding vessel. Great care must be taken to monitor for reflux of the injectate as infusion should cease before the injectate refluxes back into the main systemic artery.
- If using the microcatheter for particle delivery, consider flushing with 1000 units/mL of unfractionated heparin given the higher potential for thrombosis. This decision may depend on specific microcatheter (i.e., inner lumen diameter), estimated duration of use during the case, patient's ACT etc.). Attach the Y-adaptor to the guiding catheter and introduce the microcatheter. Place clean surgical towels under this coaxial catheter system; these will be used to contain and ultimately wrap the particle delivery catheters to prevent contamination of the catheterization table with stray microparticles.
- Advance the tip of the guiding catheter ideally at least 1-2 cm deep into the feeding vessel (Figure 2a). The tip of this guiding catheter is an important landmark. Advance the microcatheter distally into the feeding vessel.
- Particle slurry injection: Attach the stopcock to the microcatheter and gently agitate the particle slurry between the reservoir and delivery syringes (use similar technique as for contrast-enhanced echocardiograms [i.e., bubble studies]). De-air the microcatheter, then slowly inject the slurry under fluoroscopic guidance, ensuring that only the distal vessel opacifies. Flow through the vessel will become increasingly sluggish as the particles occlude the distal branches. Continue the process until the slurry begins to backwash toward the feeding vessel. Particle injection should cease when the slurry backwashes to the tip of the guiding catheter (Figure 2c). Ceasing injection at this point ensures that particles do not reflux into the feeding artery/systemic circulation.
- Remove the microcatheter, flush with saline (ideally cover end with gauze to contain the particles) and wrap the catheters in the surgical towels. Perform a follow-up angiogram through the guiding catheter to assess SPC occlusion. If needed, repeat the procedure.
Tip 4. Potential Complications and How to Deal With Them
Most important is ensuring that the particle slurry does not reflux into the major systemic artery from which the feeding vessel arises (e.g., subclavian artery, aorta, etc.). This is accomplished as detailed above. Systemically embolized particles cannot be retrieved.
Microcatheter occlusion – As previously described, delivery of PVA particles is optimized when the particles are in a suspension (i.e., not sinking or floating in the injectate). The operator needs to regularly inspect the reservoir and delivery syringes to ensure the particles remain suspended. If the particles are significantly aggregated, start by re-agitated the two syringe and then observe. As above, if the particles sink or float in the reservoir syringe, then follow the steps above to reestablish a suspension. The syringes and microcatheter will become occluded with particles if they are in an aggregate clump.
Perform close and repeated neurologic examination after the procedure. Have a very low threshold to obtain advanced imaging if any CNS abnormalities are detected.
Summary:
Particle occlusion is an effective technique to occlude SPCs. The technique is particularly important in patients with complex SPC networks or recurrent SPCs, as outlined in Figures 2 and 3. The operator must have knowledge of the patient's anatomy and ensure that all appropriate equipment is available. The critical aspects of the procedure relate to understanding the arterial anatomy and ensuring particle delivery in the intended vessel is safe. The methods outlined above will minimize the risks of complications such as systemic embolization of particles.
Figures:
Reproduced (per journal rights of authors) from Batlivala SP, Briscoe WE, Ebeid MR. "Particle embolization of systemic-to-pulmonary collateral artery networks in congenital heart disease: Technique and special considerations." Ann Pediatr Card 2018;11:181-6.
Figure 1: Particle occlusion equipment.
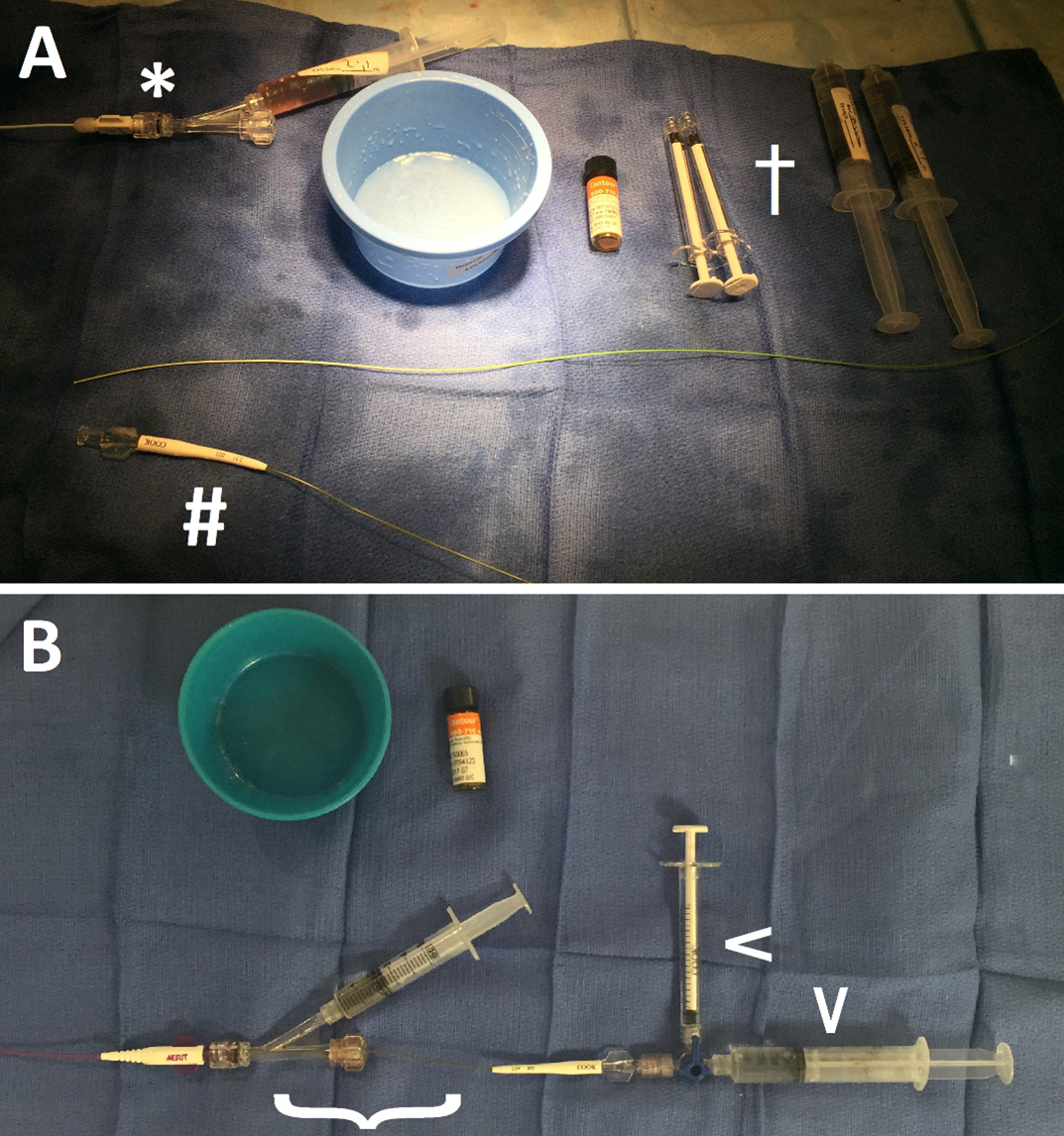
(a) The equipment is all separated. A hemostatic adapter has been attached to the 4Fr guiding catheter (*). The microcatheter (#) is prepared for insertion through the guiding catheter and into the feeding vessel. A 10mL "reservoir" and either 1 or 3 mL injector syringes are present and marked (†).
(b) Fresh surgical towels have been placed under this coaxial catheter system. The microcatheter is coaxially loaded through the guiding catheter ({). A 3‑way stopcock, with the reservoir and injector syringes attached (arrowheads), is affixed to the microcatheter.
Figure 2: Reconstituted SPCs after prior coil embolization of the feeding vessel
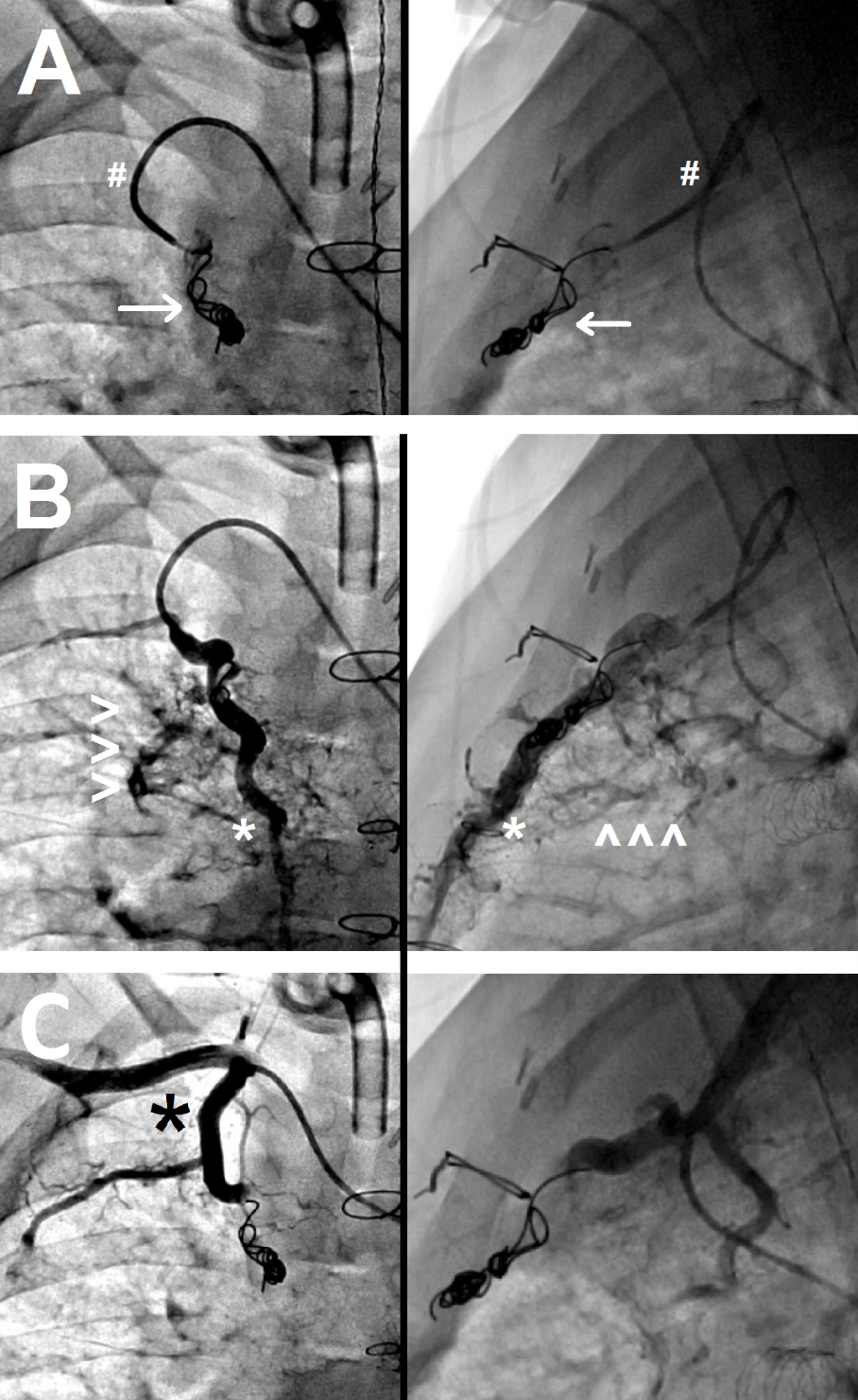
(a) The tip of the guiding catheter is ~2cm deep into the internal mammary artery (IMA) (#). Note multiple coils (arrow) in the mid‑IMA after previous coil occlusion.
(b) The IMA distal to the coils has reconstituted (*), giving rise to additional SPC networks (arrowheads).
(c) Post-particle injection shows no residual SPC flow with a patent IMA (*)
Figure 3: Occlusion of "complex" systemic-to-pulmonary collaterals.
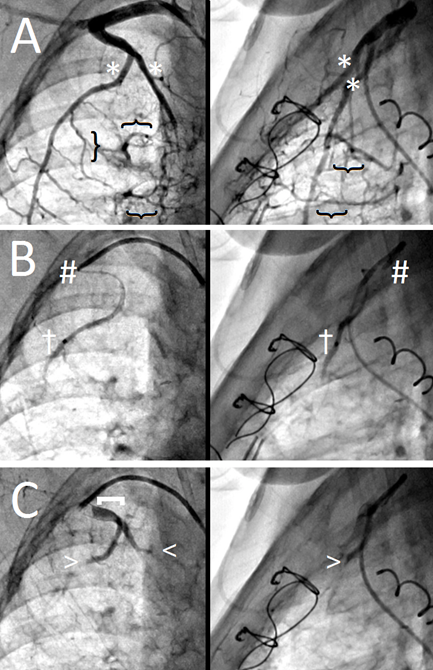
(a) Note the two large branches (*) of the internal mammary artery (IMA) that give rise to multiple SPC networks (}).
(b) The two large feeding branches are individually engaged with the microcatheter for selective particle delivery (†); the guiding catheter tip remains ~1-2cm in the IMA as a landmark (#).
(c) Post-particle injection shows no residual SPC flow (arrowheads) with a patent IMA origin ([)
References:
1. Batlivala SP, Briscoe WE, Ebeid MR. Particle embolization of systemic-to-pulmonary collateral artery networks in congenital heart disease: Technique and special considerations. Ann Pediatr Cardiol. 2018 Aug;11(2):181–6.
2. Glatz AC, Rome JJ, Small AJ, Gillespie MJ, Dori Y, Harris MA, et al. Systemic to Pulmonary Collateral Flow as Measured by Cardiac Magnetic Resonance Imaging is Associated with Acute Post-Fontan Clinical Outcomes. Circ Cardiovasc Imaging [Internet]. 2012 Jan 6 [cited 2012 Jan 28]; Available from: http://www.ncbi.nlm.nih.gov/pubmed/22228054