Author: Stephen T Dalby, MD; Brent M Gordon, MD
Arkansas Children’s Hospital, University of Arkansas for Medical Sciences
Rady Children’s Hospital, University of California San Diego
Editors: Gurumurthy Hiremath, MD; Sarosh Batlivala, MD, MSCI; Kamel Shibbani, MD; Jacqueline Kreutzer, MD
How I do it: Tips, Tricks, and Techniques
A PICS Society education
Intentional Transcatheter Stent Fracture in Pediatric Cardiology
Intentional transcatheter stent fracture (ITSF) has emerged as a valuable technique for addressing stenoses in previously placed stents that have reached their expansion limits. Stents commonly used in congenital heart disease interventions often require further expansion to match somatic growth or changing hemodynamic needs. Prior work has demonstrated that serial dilation can help to minimize stent foreshortening and offers a more predictable and complete fracture compared to direct dilation, allowing for improved vessel expansion with reduced risk of adverse events.1-3 Mechanical characterization of overexpanded stents has shown that ultra-high-pressure balloons can achieve controlled fracture, enabling further dilation while mitigating complications such as aneurysm formation.4
Despite its utility, ITSF requires careful consideration of stent type, expansion characteristics, and fracture patterns to optimize outcomes. Bench testing and in vitro studies have highlighted how different dilation techniques influence stent shortening, structural integrity, and fracture predictability.5 Clinical follow-up data suggest that intentional longitudinal and side-cell fractures can be performed safely, particularly when addressing pulmonary artery and aortic stenoses.6-8 This article provides a step-by-step guide to performing ITSF, incorporating key insights from experimental and clinical research to optimize procedural success while minimizing complications.
- Patient size. Smaller patients may have limited vascular access options and smaller vessels, thus limiting the ability to deliver necessary large-diameter, ultra-high-pressure balloons (UHPBs). Additionally, smaller vessels may be at increased risk of vessel trauma or rupture.
- Stent material. The composition of the stent directly influences the likelihood of successful fracture. Stents made of softer materials, such as stainless steel, may fracture at lower pressures, while more rigid alloys, like platinum-iridium or cobalt-chromium, often require significantly higher balloon pressures.
- Vascular access. In pediatric patients or those with prior interventions, vascular access may be restricted due to limited vessel size, occlusion, or stenosis. Additionally, repeat catheterizations can increase the risk of thrombosis, scarring, or loss of viable access sites over time.
- Napkin ring formation. Napkin ring formation can occur with significant stent foreshortening. This phenomenon can result in incomplete vessel expansion, leading to persistent stenosis and increased difficulty obtaining desired stent fracture. Ultimately the stent may need to be surgically addressed to adequately relieve the stenosis.
- Vessel damage. Excessive oversizing or uncontrolled fracture can lead to complications such as dissection, aneurysm formation, or vessel rupture. Additionally, in cases where the vessel has undergone prior interventions, fibrosis or calcification may alter its response to high-pressure dilation, and this unpredictability could increase the risk of injury.
- Surrounding structure damage. Stents placed near the airways, coronary arteries, or the aortic wall require meticulous evaluation before attempting stent fracture.
- Access. Critically evaluate vascular access sites to ensure patency and ability to accommodate sheath sizes necessary to deliver UHPBs. Stent location will dictate location of access, and care must be taken when larger arterial sheaths are required.
- Imaging. Echocardiography may be useful in determining the hemodynamic effects of the stent narrowing and necessity of stent fracture, while advanced imaging can provide additional detail regarding the surrounding anatomy and any evidence of existing vessel wall injury from prior stent implantation.
- Stent characteristics. Understanding the characteristics of the previously placed stent is paramount to performing successful ITSF. Knowledge of the type of stent, placed diameter, maximum dilation potential, and fracturability is essential
- Other. Assess patient specific factors, such as growth potential and previous interventions to better understand risks and benefits of the procedure.
- Sheaths. Sheath size must be selected to accommodate larger diameter UHPB. Long sheaths can provide extra support and ease of access for rapid stent deployment in case of residual stenosis following ITSF or vascular damage. They can also provide a means of easily performing angiography and evaluating hemodynamic response throughout the procedure.
- Catheters. Guide catheters may act as long sheaths for balloon and/or stent delivery, particularly in tortuous anatomy or smaller patients. Catheter selection depends on the vessel being treated and the stent’s location, with angled-tip catheters often required to navigate complex anatomy.
- Ultra-high-pressure balloons. UHPBs are the cornerstone of ITSF, as they generate the forces needed to fracture rigid stents while maintaining controlled expansion. Balloons such as the Atlas Gold, Conquest 40, or Athletis can reach pressures of 20-40 atm, making them well-suited for ITSF. Understanding the characteristics of the previously placed stent is essential for balloon selection. As noted by Crystal et al, serial dilation of stents versus direct dilation to maximal diameter creates a more predictable and complete ITSF. More recently, Gupta et al reported on their bench testing of various length balloons and their ability to fracture coronary stents: shorter balloons (that do not straddle the entire stent) limited stent foreshortening and allowed for ITSF at lower diameters and pressures.
- Others. Additional tools may be required depending on the complexity of the case. Specifically, having other stents and covered stents available is essential to ensure safety and efficacy of the procedure.
The catheterization procedure is generally performed under general anesthesia with endotracheal intubation in a biplane cardiac catheterization laboratory. Prepared and cross-matched blood should be readily available.
Arterial and venous access is obtained for all cases of ITSF with hemodynamics monitored throughout the procedure. Once access is achieved, 100 U/kg IV heparin is given and ACTs are monitored throughout the case to maintain therapeutic anticoagulation. Antibiotics are not typically administered unless additional stents are implanted during the same procedure.
Baseline angiography of the stented vessel is performed using advanced imaging to define optimal camera locations. Power injection versus hand injection angiography through a long sheath should be considered based on location of the stent and size of the patient.
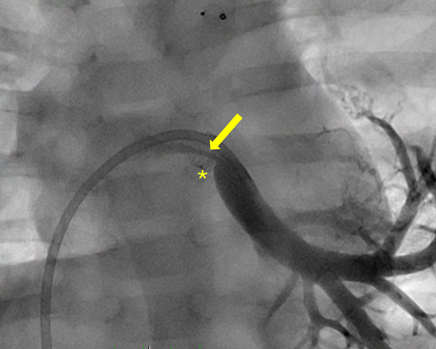
Figure 1. Frontal projection of a stented left lower pulmonary vein (*) with discrete distal stenosis (arrow) in an infant (5 mm x 8 mm Megatron DES).
Distal position through the stent is obtained using a directional catheter and wire, after which the wire is exchanged for a stiff wire that will accommodate the intended UHPB. If the stent is not yet at maximum dilating potential, serial dilation of the stent is preferred to ensure more uniform expansion and avoid napkin ring formation. If the stent has already reached maximum dilating potential or napkin ring is encountered, a suitable UHPB is selected to perform the ITSF. The diameter of the selected balloon should generally be 1-2 mm larger than the stent diameter, and often a shorter balloon will provide a more controlled dilation and fracture, as mentioned previously.
The balloon is positioned within the stent and inflated gradually under fluoroscopy until fracture is achieved. One should experience a notable tactile sensation from the catheter and inflation device, as well as a sudden resolution of balloon waist at the location of the stent by fluoroscopy.
Video 1. ITSF using 8 mm x 2 cm Conquest 40 balloon. Balloon waist is eliminated with stent fracture at 30 atm.
Angiography and hemodynamics should be repeated. Often, there will be residual stenosis of the vessel following fracture, necessitating placement of an additional, larger stent.
Figure 2. Residual stenosis of the left lower pulmonary vein following ITSF.
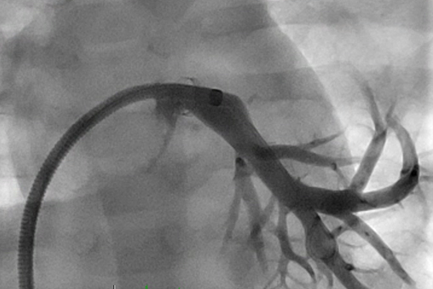
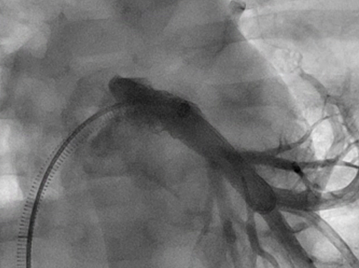
Figure 3. AP angiography following additional, larger 8 mm x 18 mm Palmaz Genesis stent
- Napkin ring formation: Napkin ring formation occurs when a stent foreshortens with dilation, creating a shortened, metallic circle that creates a vascular narrowing and obstruction to flow. This phenomenon is more likely to occur with direct high-pressure dilation or use of a long, non-compliant balloon. To minimize this risk, serial dilation with a shorter balloon – progressively increasing balloon diameter over multiple inflations – allows for more controlled dilation and fracture with less foreshortening. If napkin ring formation occurs, the stent still may be able to be fractured but typically with higher pressures and less controlled fracture, risking damage to the vessel. Once fracture of a napkin ring stent is achieved, implantation of a second stent is likely necessary to restore optimal vessel diameter and flow.
- Vascular injury. Vascular injury is a significant risk associated with ITSF, particularly in smaller vessels, previously manipulated segments, or areas of high vascular stress. Potential complications include dissection, aneurysm, vessel rupture, or thrombus formation. Careful preprocedural planning and serial dilation can help mitigate this risk, but one should be prepared to tackle this complication should it occur. Another method to potentially decrease the risk of vascular injury is to place a covered stent prior to fracture of the previously placed stent. If vascular injury occurs, management depends on the severity. Balloon tamponade with prolonged low-pressure inflation can help seal minor dissections or slow bleeding. In cases of significant injury or contained rupture, deploying covered stents can provide immediate vessel stabilization while maintaining patency. As a last option, the vessel could theoretically be embolized to prevent a life-threatening hemorrhage. In severe cases of uncontrolled hemorrhage or major vessel disruption, surgical repair may be required. Having covered stents, embolization materials, and surgical backup readily available is critical for managing these complications.
- Embolization of stent fragments. Embolization of stent fragments can occur early or late following stent implantation or ITSF. This risk is likely heightened with open-cell stents, stents with incomplete endothelialization, cases where fracture occurs in high-flow vessels such as pulmonary arteries or aorta, or in positions with repetitive force applied to the stent such as directly behind the sternum. Again, using serial dilation can help produce more controlled fracture with less risk of embolization. If embolization occurs, management depends on the location and size of the fragment. Small, non-occlusive fragments often embed in distal vessels without clinical consequences and may be left alone. Larger fragments or those causing obstruction may require retrieval with a snare catheter, bioptome, or even the ONO retrieval device.9 In rare cases, embolized fragments in critical locations may necessitate surgical retrieval if percutaneous methods are unsuccessful.
- Access. Critically evaluate vascular access sites to ensure patency and ability to accommodate sheath sizes necessary to deliver UHPBs. Stent location will dictate location of access, and care must be taken when larger arterial sheaths are required.
- Imaging. Echocardiography may be useful in determining the hemodynamic effects of the stent narrowing and necessity of stent fracture, while advanced imaging can provide additional detail regarding the surrounding anatomy and any evidence of existing vessel wall injury from prior stent implantation.
- Stent characteristics. Understanding the characteristics of the previously placed stent is paramount to performing successful ITSF. Knowledge of the type of stent, placed diameter, maximum dilation potential, and fracturability is essential
- Other. Assess patient specific factors, such as growth potential and previous interventions to better understand risks and benefits of the procedure.
ITSF is a valuable tool for managing in-stent stenosis in congenital heart disease but requires careful planning and execution to optimize outcomes while minimizing complications. The best approach to ITSF starts before the initial stent placement, selecting a stent that can accommodate future growth whenever possible. Using a stent with larger maximum expandable diameter – one that can reach adult size without need for fracture – can prevent the need for ITSF altogether. However, when fracture is necessary, serial dilation rather than direct high-pressure inflation, along with use of shorter balloons, allows for a more controlled and predictable fracture, reducing risks of napkin ring formation, embolization of stent fragments, and vascular injury. Procedural planning should also include consideration of vascular access limitations, the potential need for covered stents, and strategies for managing complications such as vessel rupture or fragment embolization. By incorporating these principles, interventionalists can maximize success of ITSF while ensuring long-term vessel patency and minimizing procedural risks.
- Danon, Saar et al. “Expansion Characteristics of Stents Used in Congenital Heart Disease: Serial Dilation Offers Improved Expansion Potential Compared to Direct Dilation: Results from a Pediatric Interventional Cardiology Early Career Society (PICES) Investigation.” Congenital heart disease vol. 11,6 (2016): 741-750. doi:10.1111/chd.12399
- Guyon, Peter W Jr et al. “Serial Dilation of Low-Profile Stents Delivered in the Aorta and Pulmonary Arteries in Pediatric Patients Leads to Spontaneous Fractures but Not to Adverse Events.” The Journal of invasive cardiology vol. 32,11 (2020): E286-E294. doi:10.25270/jic/20.00118
- Crystal, Matthew A et al. “Serial Versus Direct Dilation of Small Diameter Stents Results in a More Predictable and Complete Intentional Transcatheter Stent Fracture: A PICES Bench Testing Study.” Pediatric cardiology vol. 39,1 (2018): 120-128. doi:10.1007/s00246-017-1736-0
- Bratincsak, Andras et al. “Breaking the limit: mechanical characterization of overexpanded balloon expandable stents used in congenital heart disease.” Congenital heart disease vol. 10,1 (2015): 51-63. doi:10.1111/chd.12175.
- Gupta, Mudit et al. “Balloon Dilation Technique Influences Stent Shortening and Intentional Stent Fracture During Overexpansion of Drug-Eluting Stents: A Bench-Testing Study.” Catheterization and cardiovascular interventions: official journal of the Society for Cardiac Angiography & Interventions, 10.1002/ccd.31428. 29 Jan. 2025, doi:10.1002/ccd.31428.
- Morray, Brian H et al. “Intentional Fracture of Maximally Dilated Balloon-Expandable Pulmonary Artery Stents Using Ultra-High-Pressure Balloon Angioplasty: A Preliminary Analysis.” Circulation. Cardiovascular interventions vol. 9,4 (2016): e003281. doi:10.1161/CIRCINTERVENTIONS.115.003281.
- Krasemann, Thomas et al. “Dilating and fracturing side struts of open cell stents frequently used in pediatric cardiac interventions-An in vitro study.” Journal of interventional cardiology vol. 31,6 (2018): 834-840. doi:10.1111/joic.12549
- Agrawal, Hitesh et al. “Intentional longitudinal and side-cell stent fractures: Intermediate term follow up.” Catheterization and cardiovascular interventions: official journal of the Society for Cardiac Angiography & Interventions vol. 91,6 (2018): 1110-1118. doi:10.1002/ccd.27469
- Miller, C. E., Lim, D. S., & Shorofsky, M. J. (2025). Use of an ŌNŌ Retrieval Device for Removal of a Covered CP Stent. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions, 105(3), 597–598. https://doi.org/10.1002/ccd.31360