Author: Osamah Aldoss, MD, Bassel Mohammad Nijres, MD
How I do it: Tips, Tricks, and Techniques
A PICS Society education series
|
Szabo Technique |
The main objectives using this technique are to achieve a precise and stable position of the stent. |
The Szabo technique was initially described as a novel approach for coronary stent implantation at the aorto–ostial location. The technique utilizes a second coronary wire threaded through the proximal stent cell and acts as a retention mechanism for precise stent placement (1). Since then, multiple modifications to the technique have been applied, with some specifically for congenital heart disease (2-7). Girona et al (2) described some congenital heart disease specific modifications to the technique and classified it into different subtypes based on where the anchor wire thread is in relationship to the stent. In our field, the Szabo technique can be applied to maintain the patency of patent ductus arteriosus (PDA), to achieve a fenestration in the atrial septum, and to avoid jailing a branch pulmonary artery during right ventricle to pulmonary artery (RV-PA) conduit stenting.
This technique allows:
- Achieving stable and precise stent placement. This is applied for aorto-coronary ostial position and during PDA stenting. To attain the aim, the wire is typically threaded in the proximal stent cell. Similarly, it can be threaded through the middle cell to maintain position during atrial septum stenting to maintain half of the stent on each side of the septum (2).
- Avoid jailing important branches and maintaining access after stent implantation. An anchoring wire is passed inside the stent parallel to the balloon (between the stent and the balloon). This method was also used for coronary artery stenting to protect bifurcating branches. In congenital heart disease, it is frequently utilized during RVOT stenting to protect one of the branch pulmonary arteries (2). Less commonly, it is used during arch stenting to protect brachiocephalic arteries, most commonly the left subclavian artery.
- Cannulating the vessel of interest using the anchoring wire can be challenging if done after the stent is crimped onto the anchoring wire.
- Advancing the stent assembly through the sheath can damage the tip of the anchoring wire.
- Access - Access is dictated by the case, with no special or extra access needed.
- Imaging - Imaging is dictated by the case, with no special or extra imaging needed.
- Sheaths – The sheath used must accommodate the crimped stent in addition to the anchoring wire (typically an 0.018” wire)
- Wires – In addition to the guidewire that will be used to advance the balloon, an “anchoring wire” (typically an 0.018” wire, but other wires can be used depending on the case) will be used to cannulate a vessel of interest to allow precise deployment of the stent.
Technique: For the sake of simplicity, we will describe this method in protecting a branch PA while stenting RVOT. Two methods of delivery were used.
- The first method is to advance the whole system (including the mounted stent on the balloon catheter and the anchoring wire) through the sheath and then once in position, the anchoring wire is manipulated to cannulate the branch that needs to be protected.
- The second method is to pre-cannulate the branch needed to be protected and then mount the stent on the balloon and anchoring wire on the table before advancing the system over both wires.
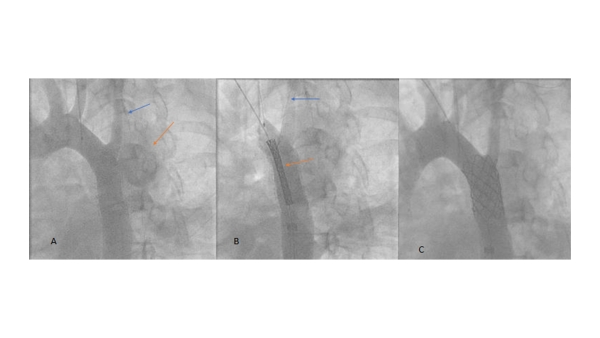
- Initial aortic angiogram shows the pseudoaneurysm (orange arrow), and its relationship to the left subclavian artery (blue arrow) (Video 8)
- Szabo technique: anchoring wire in the left subclavian artery (blue arrow), and covered stent (orange arrow) (Video 9)
- Post stent placement angiogram shows the complete covering of the pseudoaneurysm and patency of the left subclavian artery (Video 10).
The typical scenario is usually a short right ventricular outflow track where the area of stenosis is very close to the pulmonary artery bifurcation. More commonly the right pulmonary artery is the branch that needs to be protected due to the lower takeoff in comparison to the left pulmonary artery. The main guidewire will be placed in the left lower pulmonary artery. Next, the desired stent will be mounted on the balloon catheter and the anchoring wire (Figure 1). Typically, the anchoring wire is 0.018” guidewire to facilitate its manipulation under the stent. Once the stent is secured the entire stent assembly will be introduced into the long sheath that was originally placed in the right ventricular outflow tract. Caution should be practiced to avoid damaging the tip of the anchoring wire while advancing the system through the valve of the sheath. Once the stent assembly is at the tip of the long sheath in the RVOT, the anchoring wire is manipulated to cannulate the desired branch pulmonary artery to protect it in case access is needed after stent implantation (Video 1). Then, the stent assembly is further advanced as distal as possible to span the entire area of interest, including the most distal segment of the conduit. Next, the stent is deployed in the standard fashion and the balloon catheter will be removed. A repeat angiogram is obtained to determine the need for opening the right pulmonary artery. If the right pulmonary artery is completely jailed, a small balloon is advanced over the anchoring wire to dilate the right pulmonary artery (RPA). The anchoring wire is exchanged for a 0.035” wire and further balloon angioplasty is performed as needed with larger balloons.
Occasionally it is difficult to cannulate the branch that needs to be protected by external manipulation of the anchoring wire, therefore method #2 can be used where the branch PA is canulated with the anchoring wire and then the stent is mounted over the balloon catheter and the anchoring wire. The assembly is advanced inside the sheath over both wires (Video 2).
Case presentation 1: The next series of videos showed a case of a 14-year-old male with Tetralogy of Fallot who underwent a trans-annular patch with subsequent development of severe pulmonary regurgitation and very dilated RV. He was referred for transcatheter pulmonic valve placement. His anatomy was complex, including a short main pulmonary artery (MPA) segment that was amenable for balloon expanding pulmonic valve. Nonetheless, the RPA has an early take-off and is near the landing zone for the valve.
Video 3 (a and b): A main pulmonary artery angiogram A frontal and B lateral projections) through the long sheath showing the stent assembly over both wires with the anchoring wire positioned into the right pulmonary artery. The presence of the anchoring wire allowed advancing the stent all the way to the most distal segment of the main pulmonary artery. This guaranteed stenting just the entire length of the MPA without extending into the branch PA.
Video 4 (a and b): Post stent placement angiogram A frontal and B lateral projections showed a well-positioned stent capturing the area of interest.
Video 5: This showed balloon angioplasty of the jailed right pulmonary artery over 0.035” wire after an initial angioplasty using a small balloon over the 0.018” wire.
Video 6 (a and b): RPA angiogram A frontal and B lateral projections) post balloon angioplasty showed a deformity in the stent at the right pulmonary artery take-off with good flow.
Video 7 (a and b): Final right ventricular angiogram A frontal and B lateral projections) post pulmonic valve replacement showing good flow into both branch pulmonary arteries.
Case presentation 2: Another example using the Szabo technique to protect the left subclavian artery while treating an aortic arch pseudoaneurysm.
Figure 2
- A potential problem using method #1 would be the inability to cannulate the vessel that needs to be protected by manipulation of the anchoring wire. In that case, method #2 can be used by pre-cannulating the vessel followed by advancing the stent over the two wires.
- Advancing the stent assembly in method # 1 through the sheath can be challenging. Being able to advance the anchoring wire adjacent to the stent through the sheath valve can potentially damage the anchoring wire tip. In that case, using a hemostat to open the valve while advancing the system tackles this problem.
- In case of a significant covering of the branch pulmonary artery by the stent, serial balloon angioplasty might be necessary starting with a small balloon and working our way up to the desired size. The kissing balloon technique might be needed.
Using the Szabo technique in congenital heart disease interventions can be very useful. The main objectives using this technique are to achieve a precise and stable position of the stent such as in atrial septal and PDA stenting. The other objective, which is more commonly used, is to maintain access to a potentially jailed vessel by stenting. Although this method is time-consuming and technically demanding, it mitigates the risks of potential major complications that would require a much longer time trying to recanalize a jailed vessel or malposed stent.
- Szabo S, Abramowitz B, Vaitkus PT. A new technique of aorto-ostial stent placement. American Journal of Cardiology 2005;96(7a):212h-212h.
- Girona J, Marti G, Betrian P, Garcia B. Extended Szabo (anchor-wire) technique concept for stent implantation in congenital heart lesions. Pediatr Cardiol 2012;33(7):1089-96.
- Kern MJ, Ouellette D, Frianeza T. A new technique to anchor stents for exact placement in ostial stenoses: the stent tail wire or Szabo technique. Catheter Cardiovasc Interv 2006;68(6):901-6.
- Polivenok IV, Breinholt JP, Rao SO, Buchneva OV. Reverse Szabo technique for stenting a single major aorto-pulmonary collateral vessel in pulmonary atresia with ventricular septal defect. Transl Pediatr 2016;5(3):165-168.
- Salazar M, Kern MJ, Patel PM. Exact deployment of stents in ostial renal artery stenosis using the stent tail wire or Szabo technique. Catheter Cardiovasc Interv 2009;74(6):946-50.
- Lampropoulos K, Budts W, Gewillig M. Dual wire technique for aortic coarctation stent placement. Catheter Cardiovasc Interv 2011;78(3):425-7.
- Stumper O, Bhole V, Anderson B, Reinhardt Z, Noonan P, Mehta C. A novel technique for stenting pulmonary artery and conduit bifurcation stenosis. Catheter Cardiovasc Interv 2011;78(3):419-24.
Figure 1:
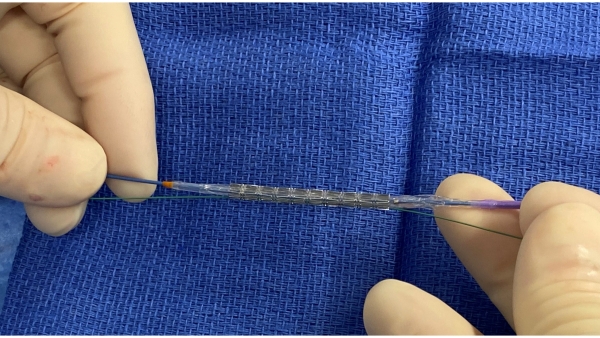
Figure 2:
Video 1:
The anchoring wire is manipulated to cannulate the desired branch pulmonary artery to protect it in case access is needed after stent implantation
Video 2:
The assembly is advanced inside the sheath over both wires
Video 3:
A main pulmonary artery angiogram (Left) frontal and (Right) lateral projections) through the long sheath showing the stent assembly over both wires with the anchoring wire positioned into the right pulmonary artery. The presence of the anchoring wire allowed advancing the stent all the way to the most distal segment of the main pulmonary artery.
Video 4:
A main pulmonary artery angiogram (Left) frontal and (Right) lateral projections showed a well-positioned stent capturing the area of interest.
Video 5:
This showed balloon angioplasty of the jailed right pulmonary artery over 0.035” wire after an initial angioplasty using a small balloon over the 0.018” wire.
Video 6:
RPA angiogram (Left) frontal and (Right) lateral projections) post balloon angioplasty showed a deformity in the stent at the right pulmonary artery take-off with good flow.
Video 7:
Final right ventricular angiogram (Left) frontal and (Right) lateral projections post pulmonic valve replacement showing good flow into both branch pulmonary arteries.
Video 8:
Video 9:
Szabo technique: anchoring wire in the left subclavian artery and covered stent.
Video 10:
Post stent placement angiogram shows the complete covering of the pseudoaneurysm and patency of the left subclavian artery.